Surgical Treatment of Chronic Proximal Rectus Femoris Rupture
Rectus Femoris Anatomy
The quadriceps muscle group is vital for athletes who participate in sports that require running, jumping and kicking.
Of the four muscles that comprise this group, the rectus femoris is the most commonly strained and also has the most complex anatomy.
The rectus femoris goes from the hip to the knee and can be used to straighten the knee or lift the knee up.
The rectus femoris muscle is the most anterior and superficial of the quadriceps muscle group.
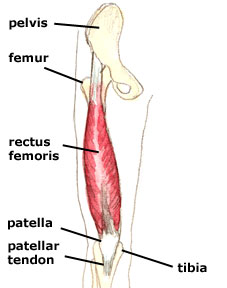
The other components of the quadriceps mechanism are the vastus medialis (with its distal, oblique component), vastus intermedius and vastus lateralis.

At the distal thigh, the tendons of these muscles merge to form the quadriceps tendon.
The rectus femoris acts to extend the lower leg at the knee and flex the thigh at the hip.
It is a direct antagonist to the hamstrings and it is innervated by the posterior division of the femoral nerve.
Rectus Femoris Rupture
This muscle can rupture at the upper part.
The main cause of this is overuse through kicking or explosive movements as in sprint starts.
The symptoms of a rectus femoris rupture include:
- A sudden sharp pain at the front of the hip or in the groin usually whilst doing some explosive activity e.g. sprinting, jumping, hurdling.
- Swelling and bruising may occur.
- Pain in lifting the knee up against resistance.
- If it is a total rupture then it will be impossible to contract the muscle.
- Limp when walking.
Diagnosing the Tear
The injury can be missed.
Some athletes may not seek medical attention thinking that the injury may be minor muscle strain.
Sometimes the diagnosis is difficult for the doctor to arrive at if further investigations such as ultrasound scan or MRI scan were not ordered.
Delayed diagnosis is common.
The best diagnostic test is either an ultrasound scan or an MRI scan.
Case Study
A 26-year-old semi-professional soccer player experienced a tearing sensation in his right thigh as he attempted to kick the ball. He was unable to complete the match and developed severe bruising and swelling.
He went to consult a Sports Physician who performed a bed-side ultrasound scan. He was told to have a partial tear of the ilio-psoas muscle in the groin.
He was advised to rest, take some pain medications and undergo physiotherapy.
He was reviewed in a month’s time. He reported reduction of his pain in the groin but noticed difficulty when trying to kick a ball with force. He also noticed a lump in his right mid-thigh.
The Sports Physician referred him for an MRI scan.
The MRI scan showed a rupture of the proximal rectus femoris musculotendinous junction.


He was referred to an Orthopaedic Surgeon for possible surgical repair of the ruptured rectus femoris.
It was 8 weeks by the time he was reviewed by a surgeon.
He was told that surgery was not required. He was also encouraged to seek a second opinion.
He came into my clinic at 9 weeks post-injury.
His main concern was whether he needed to go for surgery to repair the torn muscle. He had pain in his right thigh when he tried to kick a football with force. He also felt that he could not kick a football as strong as before his injury.
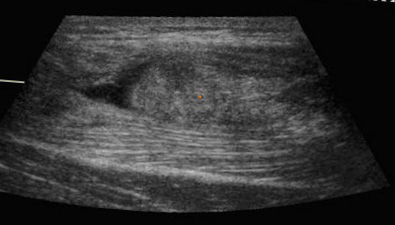
A bedside ultrasound scan in my clinic reviewed a completely torn rectus femoris and the torn end was still in the proximal third of his right thigh:
To Repair or Not to Repair?
There is no prospective randomised controlled study comparing surgical repair versus conservative treatment of rectus femoris ruptures .
It is probably acceptable not to perform surgery if the patient is not a sports-person.
Straw and co-workers published a case report in 2003 in the British Journal of Sports Medicine entitled “Surgical repair of a chronic rupture of the rectus femoris muscle at the proximal musculotendinous junction in a soccer player.”.
They described their treatment of a chronic rupture of the direct head in a semiprofessional soccer player. Their report offered objective data showing decreased function of the quadriceps and the hamstring muscles as a result of this patient’s nonoperative treatment.
The impact on the hamstrings was hypothesized to be a result of hamstring wasting attributed to a decreased need for their antagonist function.
The power and performance of both muscle groups improved to levels comparable to those of the uninjured side after repair and rehabilitation of the rectus tear.
This work suggests that the long-term effect of an unrepaired rectus femoris tear is more than cosmetic. It may lead to subjective and objective findings of weakness and loss of power: sequelae that may be intolerable to the performance athlete.
Garcia and co-workers published in the Archives of Orthopaedic and Trauma Surgery in 2012 on their case series of 10 professional soccer players in the Spanish Football League who underwent surgical treatment of proximal ruptures of the rectus femoris.
They found that surgical treatment had a lower recurrence rate. They felt that surgical treatment was indicated in these professional soccer players for a complete functional recovery.
What Was Done?
Surgical repair of his torn proximal rectus femoris was performed at 10 weeks post-injury.

The direct head was explored via an anterior surgical approach (Smith-Peterson). The rectus tendon was found to be completely torn from the anteiror inferior iliac spine (AIIS).
The torn muscle was identified and mobilised.
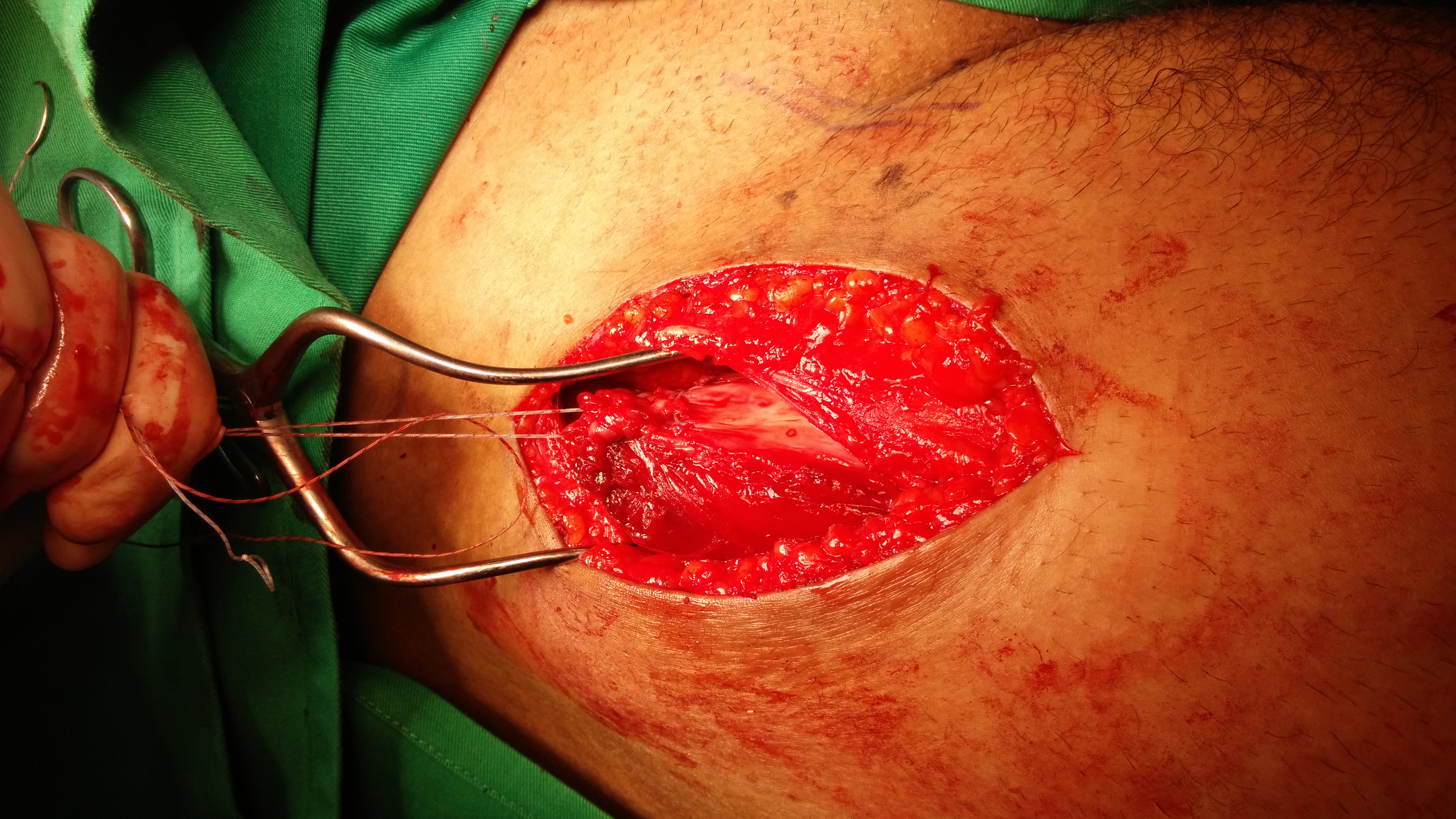


Suture anchor is applied to the anterior inferior iliac spine:
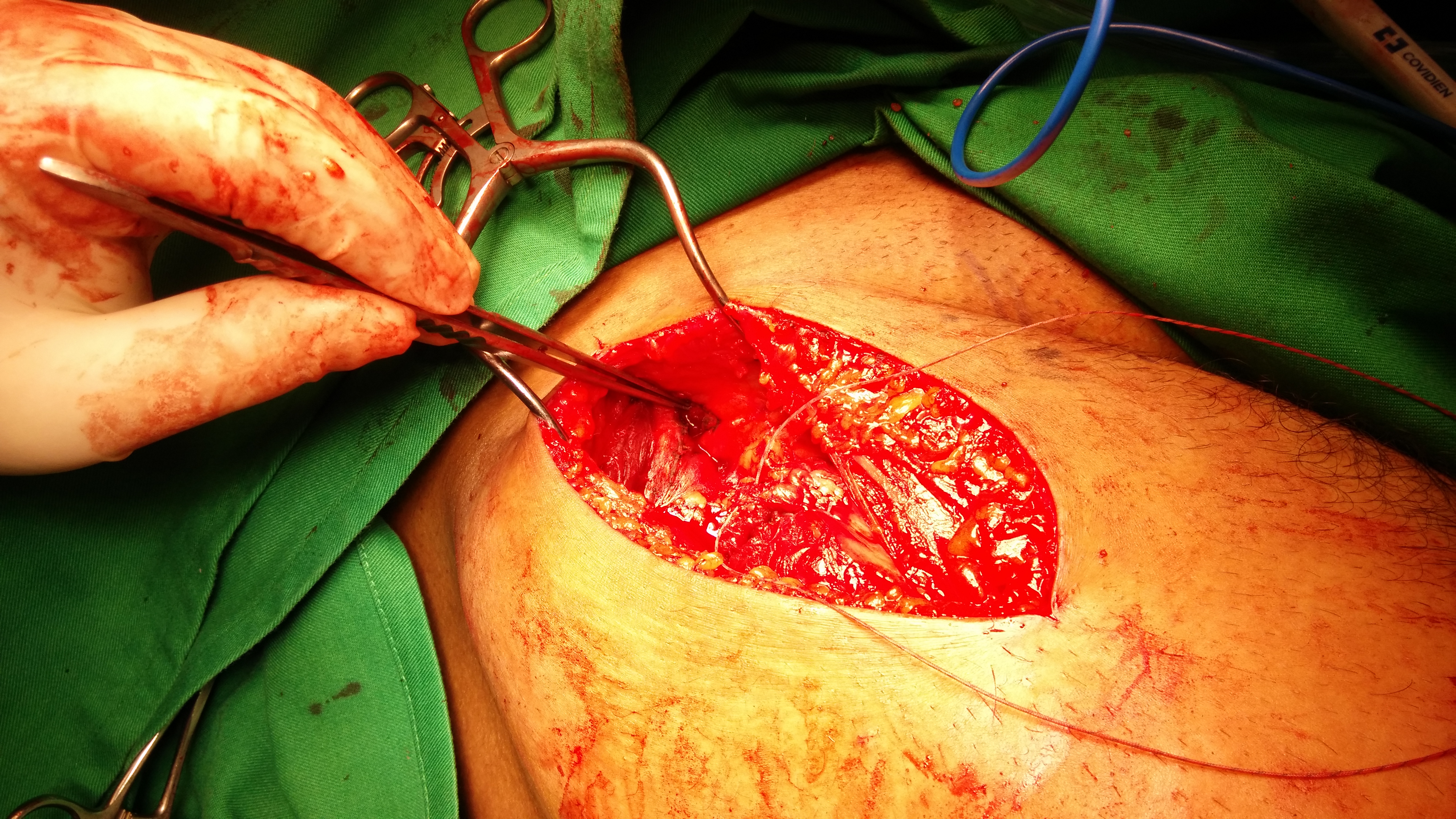

The torn rectus femoris is repaired to the footprint.

Video
Post-Operative Care
The right knee was immoblised with a knee brace locked in full extension.
He was asked to ambulate with crutches and only toe-touch weight bearing in his right leg for 6 weeks.
He was told to avoid extension of his right hip for the next 6 weeks.
He was allowed to walk full weight bearing by 6 weeks post-surgery.
For more information on rectus femoris tear and treatment, please contact Dr HC Chang at +65-683 666 36 or visit us at http://www.ortho.com.sg
