Tear of the Rectus Femoris Direct Head – Surgical Repair
Rectus Femoris
The rectus femoris muscle is one of the four quadriceps muscles that sits in the middle of the front of the thigh.
The rectus femoris attaches from the pelvis to just below the knee (on the patellar tendon.) It is responsible for knee extension and hip flexion.
The other muscles of the quadriceps include the vastus medialis, the vastus intermedius and the vastus lateralis.
It is one of the muscles that make up the hip flexors; a group of muscles that bring the legs and trunk together in a flexion movement.
| ORIGIN Straight head: anterior inferior iliac spine. Reflected head: ilium above acetabulum |
 |
| INSERTION Quadriceps tendon to patella , via ligamentum patellae into tubercle of tibia |


Rectus Femoris Injury
Injury to the rectus femoris muscle is common in athletes, second only to the hamstrings among lower extremity injuries.
It is the most common lower extremity muscle injury among soccer players.
The rectus femoris is vulnerable to injury because it crosses two joints, has a high proportion of type II, fast twitch muscle fibers and because, in an athletic kicking motion (soccer, football, martial arts), it undergoes forceful eccentric contraction while passively stretched at the onset of the forward swing phase.
The most significant of the other risk factors for muscle strain is recent or remote injury to the muscle.
Re-injury often occurs at a different location within the muscle or, if in the same region previously affected, is seen at the margin of a region of scarring.
The rectus femoris is also prone to injury if there has been recent hamstring injury. Other proposed risk factors include low muscle strength, muscle imbalance, limited flexibility, muscle fatigue, inadequate warm-up and improper technique.
The most proximal rectus femoris tendons may be injured at or just distal to their origin.
The same mechanism of injury in a skeletally immature athlete results in avulsion fracture of the AIIS, at the origin of the direct head, owing to the vulnerability of the open apophysis.
Rectus femoris muscle injury usually consists of a myotendinous strain centered on the indirect or direct head or, less commonly, myofascial junction injury, at the periphery of the muscle.
The majority of rectus femoris injuries occur about the deep intramuscular musculotendinous junction9. Other injuries to the quadriceps mechanism include muscle contusion, vastus muscle strain, distal rectus femoris musculotendinous junction strain and quadriceps tendon tear.
Rupture of the rectus femoris
The rectus femoris is one of the powerful quadriceps muscles. A rupture of the tendon at the top of the muscle near the hip can result from overuse or explosive loads on the muscle such as in kicking or sprinting. .
Inflammation of the muscle causes pain in the groin during physical exercises that use this muscle.
The patient may experience pain during knee raises when the muscle is ruptured or inflamed.
An operation may be necessary if the muscle is torn.
Ruptured rectus femoris tendon symptoms
- Symptoms include a sudden sharp pain at the front of the hip or in the groin usually whilst doing some explosive activity.
- Swelling and bruising may occur with pain when lifting the knee up against resistance.
- Tenderness will be felt when pressing in at the muscle attachment at the front of the hip.
- If a complete rupture has occurred then it will be impossible to contract the muscle.
Case Example
A young man experienced some minor right groin pain with sporting activities over the past 1 month. He continued to engage in sports despite the occasional right groin pain or discomfort.
He was playing football when he felt a muscle over the front of his right hip “tear”. He had sudden onset of right groin pain and was unable to continue running.

Examination showed tenderness over the front of his right hip and proximal right thigh with weakness in right hip flexion.
A clinical diagnosis of a possible right quadriceps muscle tear was made.
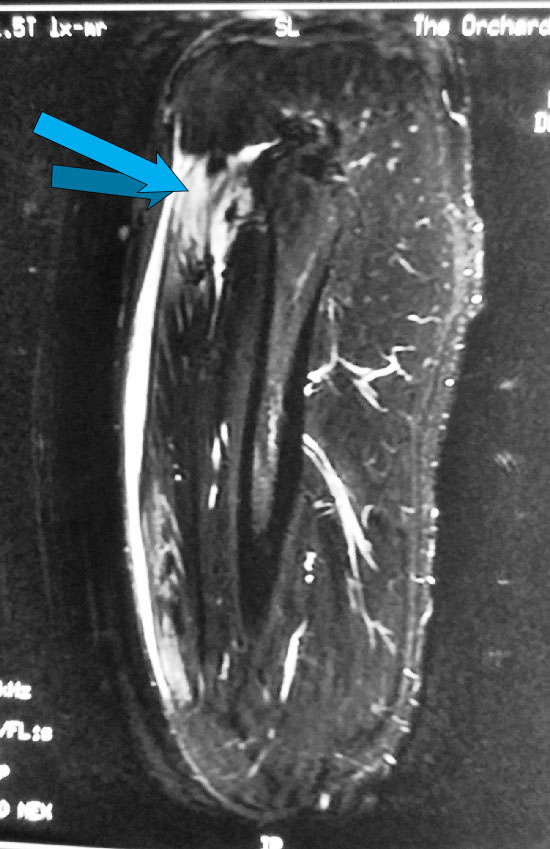
An MRI scan of his right thigh was ordered. The MRI confirmed a tear of the direct head of the right rectus femoris.


He was offered surgical repair of the torn rectus femoris.

A 6 to 8cm longitudinal incision was made just lateral to the anterior superior iliac spine (ASIS) and moving distally.
The lateral cutaneous nerve of the thigh and the branches of this nerve were identified and carefully protected during the surgical exposure.
The plane between the sartorius muscle and tensor fascia lata was developed.

The torn rectus femoris tendon was found.

The torn tendon was reattached to the anterior inferior iliac spine.
The surgery is shown in this video:
Postoperatively, passive range of motion was initiated for the patient’s hip for 4 weeks, with weightbearing (as tolerated) in a knee brace locked in extension. He started active range of motion at 6 weeks after surgery. He was able to participate in sports (including sprinting) without any limitations by 3 months post-surgery.
For more information on rectus femoris muscle tears and the treatment, please visit us at http://www.ortho.com.sg or email us at hcchang@ortho.com.sg

Is it possible that a surgeon can with surgery accidently nip/ cut femoralis rectus muscle while taking out a neuroma and adhesions, while doing a neurectomy of lateral cutaneus nerve? I had surgery 10 days ago and from the beginning has pain upper leg and difficulty walking and a sudden sharp tearing” sound one day when i got out of bed, now i have painfull upper leg and constant pain can walk?
Hi,
It is possible but highly unlikely as the lateral femoral cutaneous nerve of the thigh and the branches are superficial to the fascia of the rectus femoris.
hc
Hello,
I believe I tore my rectus femoris about a year ago while sprinting outside during soccer training. I since have not seen a specialist and have been injuring the spot continuously since due to a lack of proper therapy. It does not hurt when I sprint or run, only if I kick a soccer ball really hard without first warming the muscle up. Should I continue to strengthen it with weightlifting or would that be a bad idea?
Hi Abdullah,
You should consider working with a physiotherapist to reduce the pain and improve the strength.
Regards,
hc
Hi,
I have a complete tear my rectus femoris muscle proximal to it’s insertion on the patella with 6.6 cm retraction. Because I can still extend my knee without any problem, am relatively pain free and have still have most of the strength in the affected leg, my doctor feels I should not have surgery. He says that there may be very little tendon to reconnect and, as he put it, you can’t sew muscle. He said the lump will gradually decrease in size and that that there would be no long term disadvantages to not having surgery. Do you agree?
Thank you,
Dear Brian,
This is controversial. It is not possible for me to advise you over the net. I have successfully repaired such tears in the past but I also have patients who have done quite well without surgery. You need to discuss it with your own doctor.
Regards,
hc
Thank you very much for your fast reply. I’m truly appreciative.
I injured my quad a little more than three years ago. It was originally diagnosed as a strain but the pain never ceased and the lump in my thigh got bigger. 9 months after the injury, an MRI was performed and showed it was torn. After two years, I was finally able to see an O.S. and the result of the new MRI was Abnormal origin of the right rectus femoris as compared to the left rectus femoris. The proximal myotendinous junction is 6 cm caudally displaced as compared to the left and there is decrease in bulk of the proximal musculature as compared to the left. There is some edema at the myotendinous junction as well. The assessment was a chronic proximal quadriceps avulsion from the pelvis. I’ve been in regular physical therapy for nearly a year and a half and nothing has changed. I still have a large lump in the thigh and any sort of use of the muscle causes pain. I was told that it would be inoperable at this point and I’m trying to find other opinions about my injury. I find it hard to believe that there aren’t any options to treat this and that I’ll be left with limited use and constant pain for the rest of my life.
HI Jason,
The diagnosis need to be accurate and arrived at promptly once you present with the injury. Once it is more than 3 months post-injury, it is impossible to repair the tendon back to the bony attachment due to contractures.
Regards,
hc
Not the answer I was hoping for but one that I expected. Thank you for your reply.
Dear Dr Chong
I had a hip arthroscopy in 2015. Now im suffering of scar tissues in the musscle straight head of rectus femoris. Is it recommended to remove chronic scar tissues with open surgery?
Have you ever perform such an operation?
Thank you
Dear Antonis,
I have not come across such a problem before.
Regards,
HC
My 11 year old son injured his left hip last week after playing kick ball. He feel, felt a “pop” and was unable to bear weight. There seemed to be some protrusion of the left hip at that time. He later sat in a wheelchair at the ER and the pain went away and he felt the hip was ‘back in place’.
8 days later he had MRI which indicates an an avulsion
fracture at the anterior inferior iliac spine at the attachment of the rectus femoris. There is a
complete tear of the main part of the rectus femoris (direct head) and probably partial tearing of the
lesser part (indirect head) with 3-4 mm retraction with bleeding (hematoma) at the site. Also seen is
a strain of the iliopsoas at the attachment at the lesser trochanter just below the hip joint, but no
tear here.
He has some mild pain with long distance running, otherwise has no complaints.
Could the reading of the MRI be wrong? Why isnt he having pain?
What will his treatment be?
I have a very disappointed boy who has been told he cannot play baseball- and the season is just beginning…
Hi,
A lot of young patients have such injuries and recover well with conservative treatment.
Regards,
hc
I Had an Total right hip replacement last Nov. 15, 2017. It was an atherion incision, how ever the rectus femoris was teared during the surgery (Not an accepted complication) I am a 71 years old male fairly active and working still. would you recommend the muscle repair that now is separated from the lesser trochanter 5″ or more now? If yes: what type, and name of the surgery? Thank you. 🙂
Hi,
The rectus femoris does not attach from the lesser trochanter.
Regards,
hc
Oh whoa! Than it looks like that the doctor that read my MRI about three month ago was mistaken… Furthermore my present surgeon told me that I have a complete rectus gemiría tear (Approx 5”) at the level of the lesser trochanter… it was grade 2 … Are they both wrong? My pain persist … today is my 71st birthday, and I am not even able to play golf fro the consisten pain right at my right hip joint 😦
Thank you for your kind reply… RSR
Can a Rectus Femoris Avulsion Fracture cause muscle fatigue in the leg?
Hello Dr. Chang Haw Chong,
Summer 2012 age 36: While playing softball I slid head first across home plate; in my excitement I exploded to my feet by pushing off the ground hard enough to pull my feet under me and land upright, something I’d been doing for 20yrs. I felt the rupture instantly in the proximal lateral part of my right thigh. Additionally, over the next few days, pain began radiating from the proximal but more medial portion of my left thigh. I limped through the next few weeks until large contusions/blood/adema formed above my knees. I had no insurance at the time so I limped on. The fluid filtered away and after a few months I was able to “function”
Summer 2014: Changed careers and started a small(me only) construction company, which caused my leg muscle use to increase exponentially. Pain returned in both legs and right hip. Made appt w/ my regular Dr. He ordered MRI on right quad and left groin areas. A couple weeks later he and I sat to discuss results, He confirmed a tear of proximal end of right Rectus Femoris. I cant remember if it was the tendon or muscle or the severity? Also, he informed me that MRI didnt get enough of my left quad to see a tear, but based on the similar divots in both quads and the blood that drained down to both knees weeks later, we determined that I most likely suffered a partial tear to the left RF also. He advised me of my options. I decided to do some home phys therapy and tough it out mainly because of the two year delay and financial strains of a new business.
Winter 2017: While pushing myself through a huge job I developed severe bursitis, tendonitis, and mild arthritis in both already beat up knees. I stopped using them and began bending at the waist for everything….really bad plan. The overuse of the related muscles combined with the quad injuries caused severe pain and spasms in my pelvic and lumbar areas, which stopped my everything! Self Diagnosis: Symptoms were exactly as described from Ilio-psoas syndrome
Winter 2018: 18 PT sessions restored the use of my knees and muscle relaxers/anti inflammatory meds made it possible to “function” again.
Winter 2019(current) age 44: I was taking more and more muscle relaxers each month so I quit them 3 months ago. It seems like I’m losing a little more of my ability to “function” each week, and this is a time I need to excell not merely function. The severity and regularity of my pain is taking a toll on my everything lol. Current symtoms: Recent X-rays show pretty significant anterior movement of my L4 vertebrae and severe anterior tilt of my pelvis, severe flexion of low back. It seems my lower lumbar is constantly in a state of spasm, happens every day with varying severity. I believe this is due to my (now)hyper strong psoas, hip flexors, etc.. which is my bodies compensation for the lack of help from my torn RF’s??
…..and that’s not my biggest problem. I believe I’m also suffering from Pudendal Nerve Entrapment caused by Piriformis Syndrome, and it is far far more disruptive than lumbar spasms. Ilio-psoas was more painful but within a week I discovered I could stop the spasm immediately by tightening my opposite oblique. I have found no release trick for the burn of the Piriformis spasm.
I apologize for the long-winded back story but I wanted you to have as much info as possible in hopes you might be able to offer some thoughts/suggestions?
My questions for you are: 1. What muscles would most likely compensate for the torn RF muscles?
2. Is it likely(or plausible) my torn RF muscles are the root cause of all my problems?
If they are, 3. What else should I be concerned about having problems with in the future? Hip sockets? sacro-iliac joints? knees? etc..
lastly, 4. What do you recommend I do now?
thank you, sincerely, Dan
Do you have any other information on the direct or so indirect head tear of the Rectus Femoris during Total Hip Replacement?
How timely does surgery need to be for a fully torn rectus femoris. My son just tore the rectus femoris in both legs at a trampoline gymnastics competition (based on MRI today). Is this like other tendons when surgery needs to happen within a few days? Thank you!
I ended up have the rectus femoris completely detach from the pelvic area and not having it properly diagnosed, i went a year before getting an MRI, by then it had reattached itself lower having shortened and producing a calcium deposit under the rectus femoris. I decided to just have the calcium deposit removed and to not have it reattached back in its correct spot. its been several years and the difference has caused a major imbalance in my right side (the side of the injury) so when i squat it forcefully shifts my weight to the injured side due to it being attached lower. am i able to do anything to fix this? i have slight OCD and uneven things drive me crazy and im horribly uneven and losing my mind.